
The Rise of Fentanyl
We speak of the US opioid epidemic as if it is one single thing, but it is actually a rapidly shifting, regionally variable wave of different events. We are currently in what many consider to be the 4th wave of the opioid epidemic: use of high potency synthetic opiates (i.e. fentanyl and its friends) + stimulants (methamphetamine or cocaine) along with some special flourishes like Xylazine. The reason I say this is regional is because new drugs do not hit all areas of the US at once. They tend to enter in one area and sort of spread/diffuse into others. For example, fentanyl came in first to the Northeast US. This is because the Northeast long sourced heroin from areas that supplied it in the white powder form compared with places like the West Coast which tended to be more frequently supplied with black tar heroin. It was easier to mix the white powder fentanyl into the white powder heroin. For this reason, graphs of the overdose deaths of the US tend to show fentanyl hitting around 2013/2014 but in my area in North Carolina we didn’t start seeing it as much until a few years later. The amount of additives like xylazine will also vary place to place; nearly all of the fentanyl in Philadelphia is laced with xylazine but it is much less in other areas. Why does fentanyl matter? Fentanyl is more potent than heroin so less drug is needed to get the same effect. Fentanyl is also supposed to have a very short ‘half-life’ meaning its effects should wear off and the drug leave your system fairly quickly. This is somewhat true-persons who use fentanyl do tend to feel that the effect wears off quickly and have to use more often. BUT. We have found that when persons use large amounts of fentanyl regularly that something interesting happens. Fentanyl loves fat and it seems that with a lot of use the fentanyl can sort of deposit into your body’s fat stores. Then when you stop using the fentanyl it can slowly release from the fat into your system at low levels. Case reports show urines testing positive for fentanyl weeks after last use.
How We Used To Do It
In order to understand why fentanyl is making buprenorphine inductions harder, that we have to look at how we used to do inductions and why.1 Remember: buprenorphine always wins. It will push any other opioid that is present in your system out of the way, off of the opioid receptor. But even though buprenorphine is stronger in THIS way, once it takes the place of the old opioid it turns the ‘volume’ down from 100% to 50%. This drop from 100% to 50% is withdrawal which we have caused (‘precipitated’) by giving you the buprenorphine. In order to avoid precipitated withdrawal in the past we would have you wait a few hours after your last use of prescription opioids/heroin until you felt moderately unwell, give you a small amount of buprenorphine, and slowly increase the buprenorphine over 2-3 days. People got on buprenorphine after experiencing only a few hours of mild-moderate withdrawal symptoms. Why did this work?
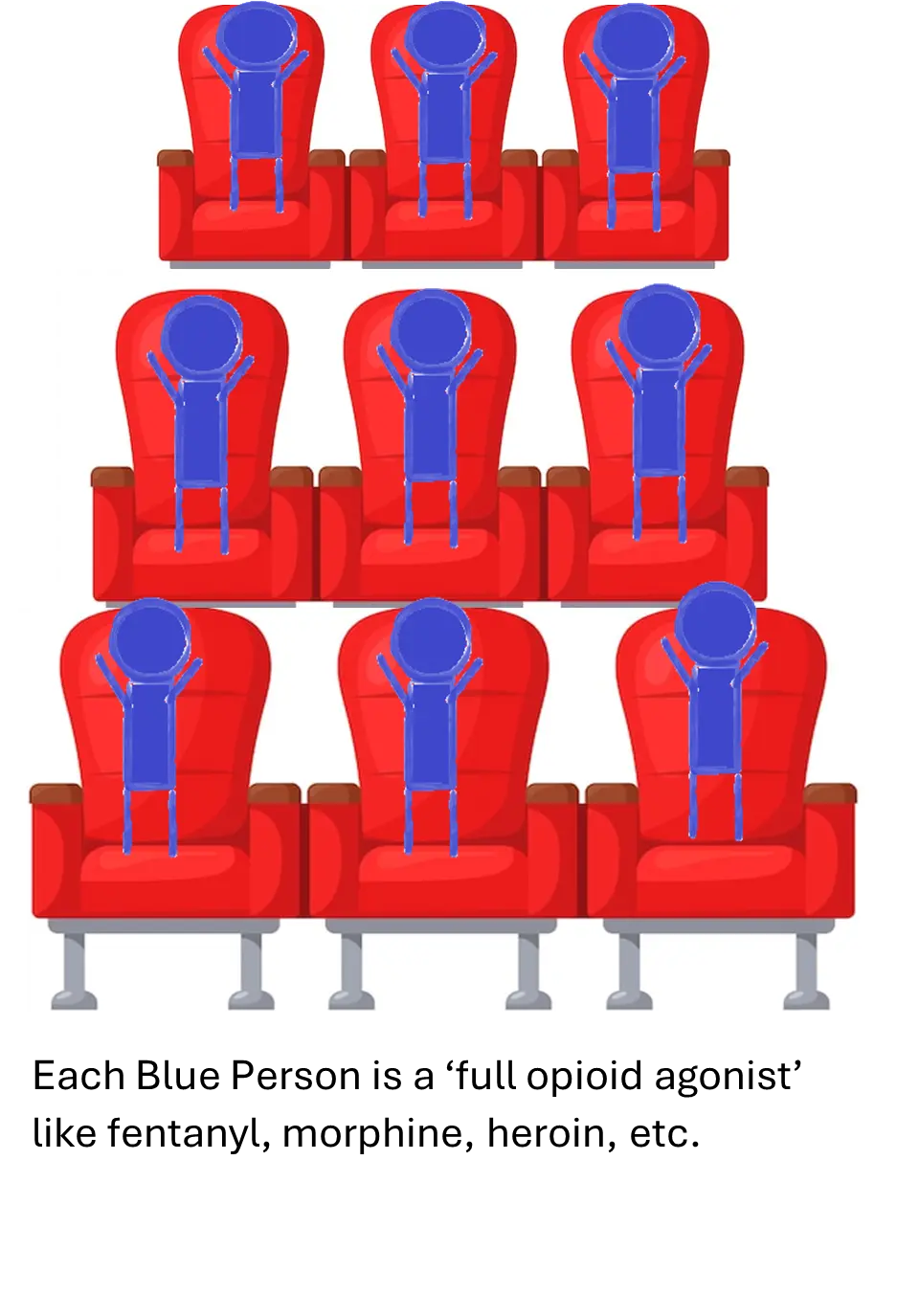
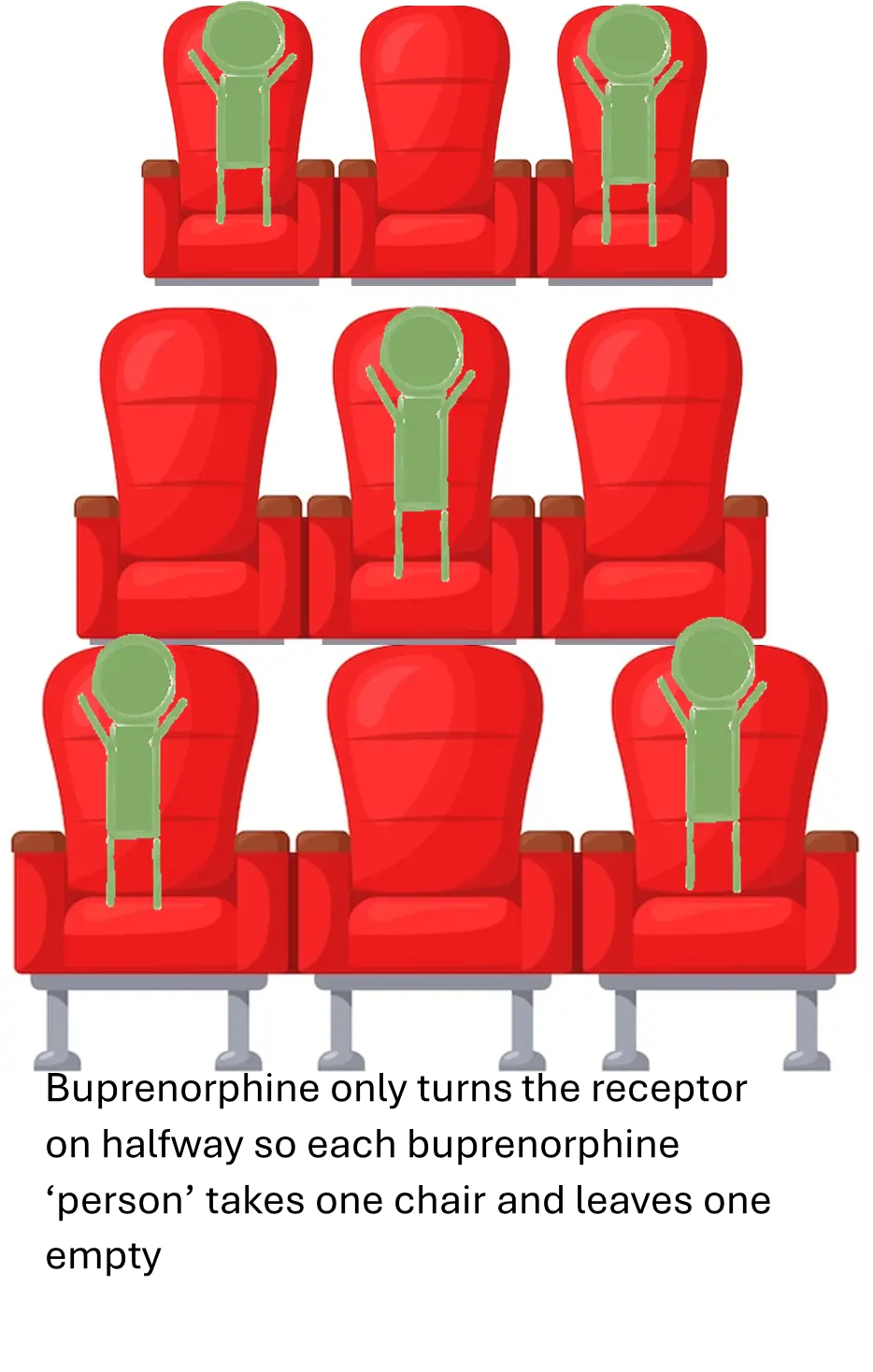
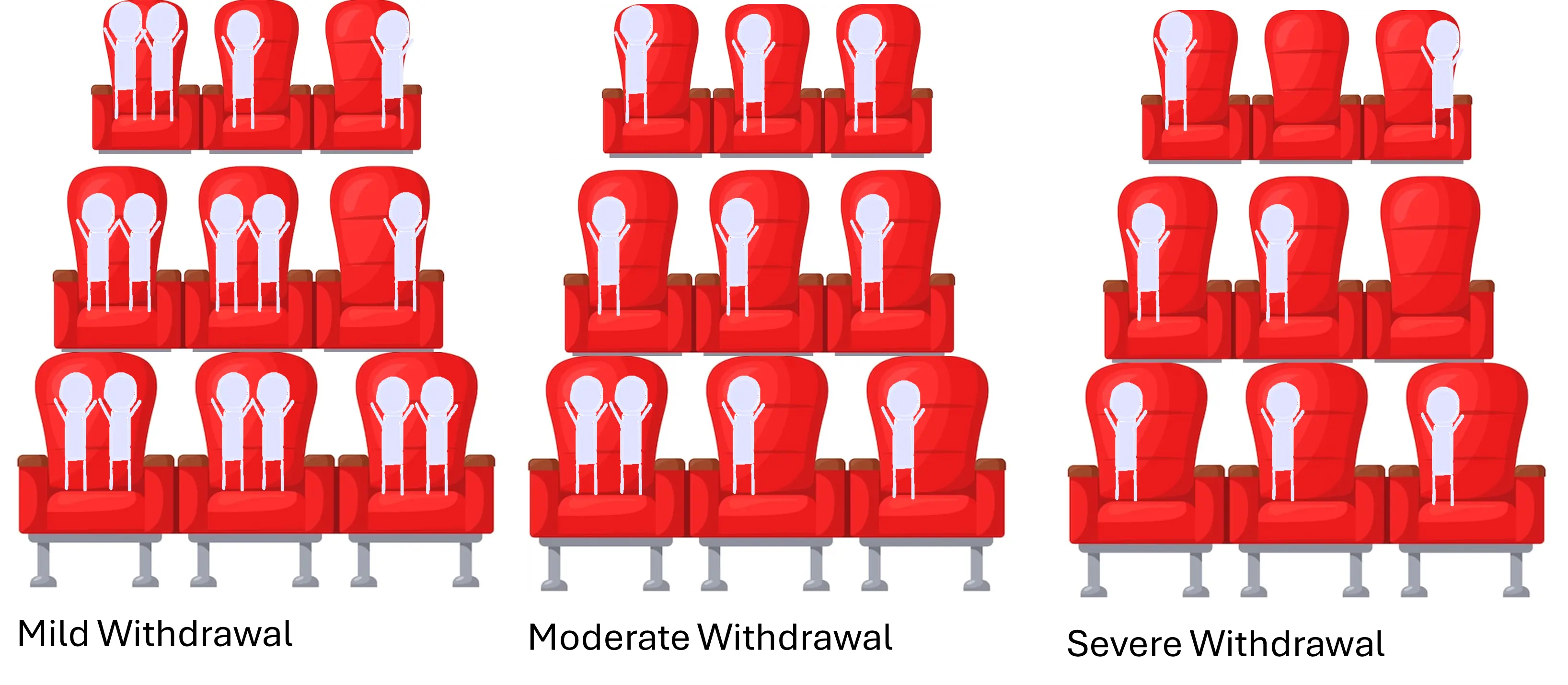
Well Imagine your brain opioid receptors are like the seats in a movie theater-each chair is an opioid receptor in your brain. Imagine when I give you hydromorphone, heroin, methadone, etc. it is putting a person in the chair. In advanced addiction, the person feels ‘normal’ and not sick when the receptors (chairs) are filled. Buprenorphine is different. It only turns the receptor on halfway. So to visualize that lets imagine that each time a buprenorphine sits down it causes the neighboring chair to go empty.
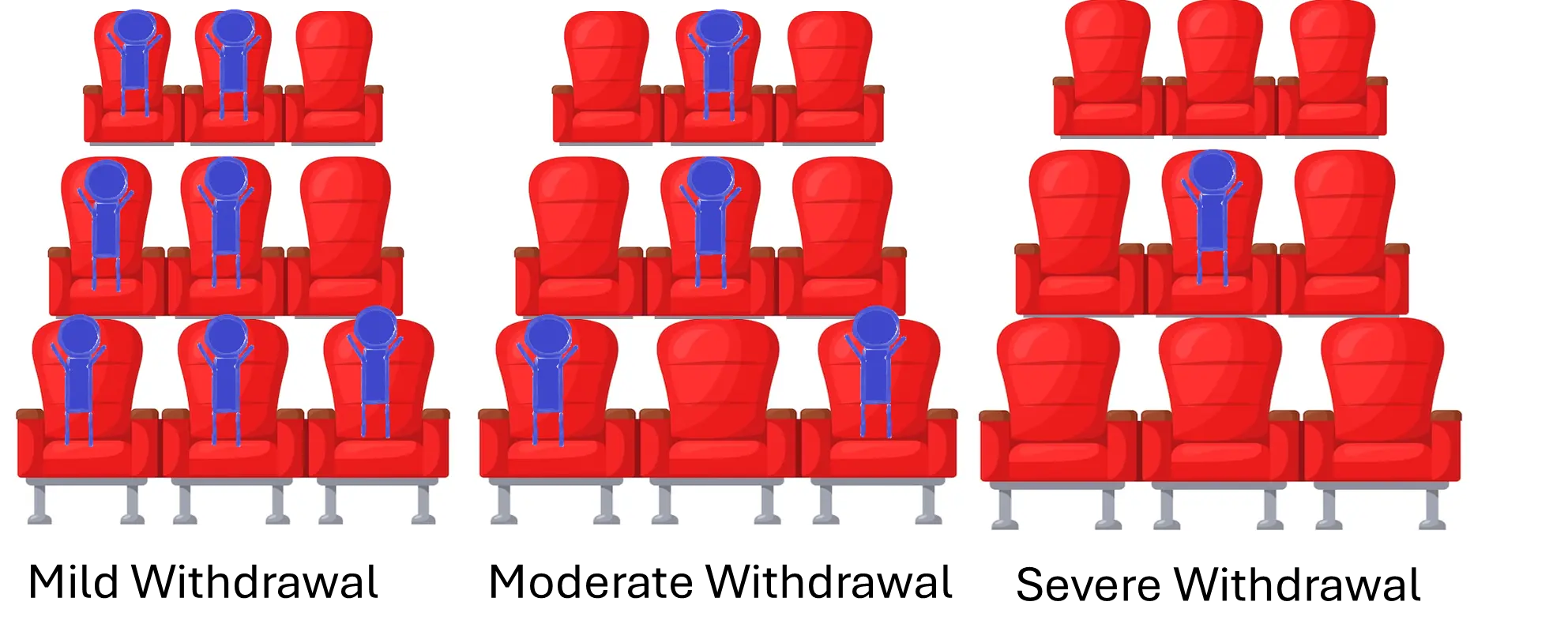
So. Imagine you just used a full opioid like heroin. Your theater looks like the picture on the left above and you feel pretty good/normal. As time goes by the drug wears off: these guys get up and leave their seats empty. More empty seats= more withdrawal. Different drugs have different speeds at which people leave the seats. Heroin and hydromorphone leave their seats faster than morphine which leaves faster than methadone. In the cycle of addiction the person uses every time enough drug has left enough ‘seats’ empty that withdrawal is kicking in.
Now. Let’s think about what happens if we add buprenorphine to the mix. REMEMBER: Buprenorphine always wins: if there are no empty seats, buprenorphine will grab the seat, kick the other guy out, and take its place. And for each seat the buprenorphine takes it leaves a seat empty. So what does this look like if we take buprenorphine (Bup) at each of these stages above.
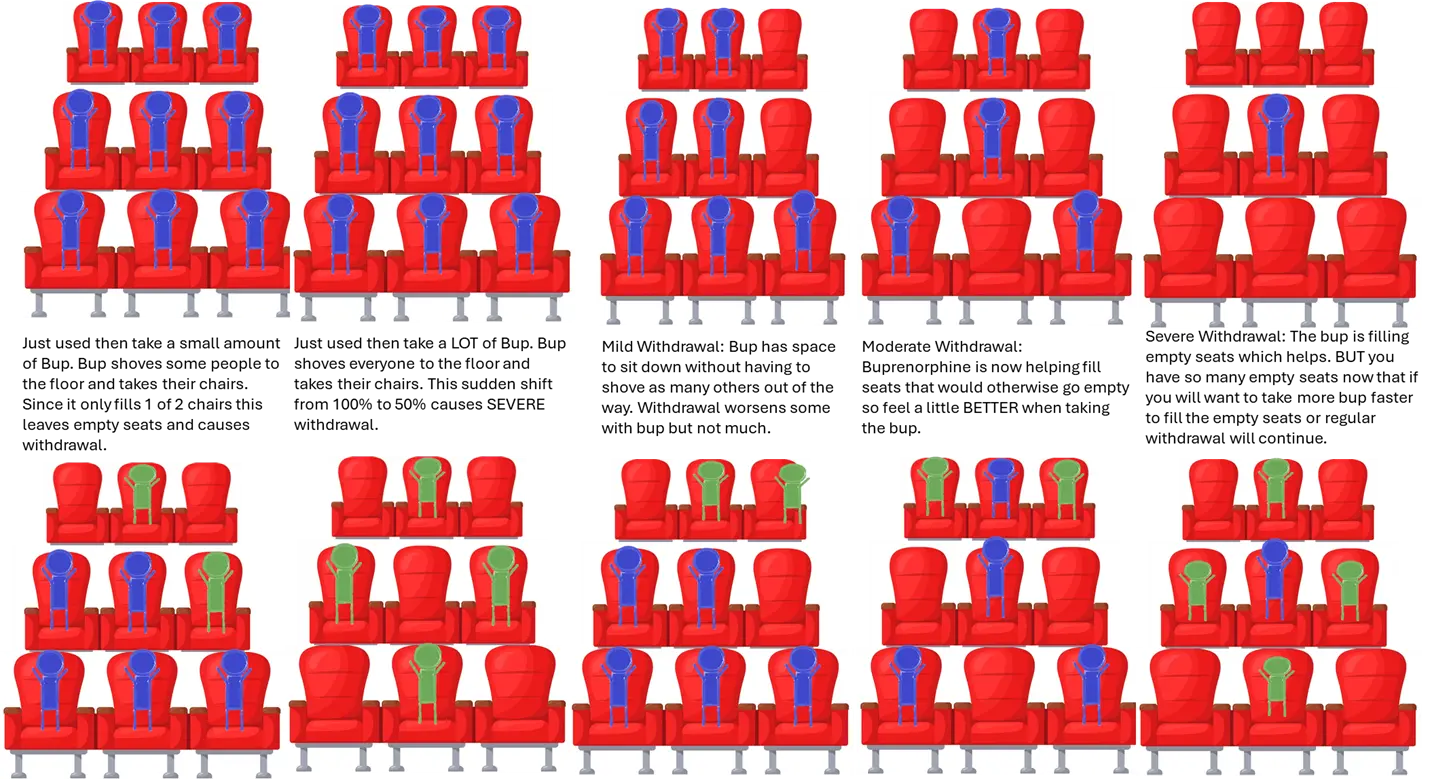
So now we see why this approach worked: people would wait until they were in moderate withdrawal and take a small amount of buprenorphine. They would then feel BETTER with the buprenorphine and more comfortable. They then felt well enough to wait another hour or 2 for more seats to empty and would then take more buprenorphine. By the end of 2-3 days all of the seats were filled with buprenorphine and the person did not have any withdrawal symptoms. It is all about keeping the balance: wait just long enough for open seats to become available so taking buprenorphine helps us feel better rather than worse but not waiting so long that someone is in severe withdrawal feeling awful.
Fentanyl Gumming Up The Works
Fentanyl throws off the balance because it is more potent than heroin. You need a lot less fentanyl (maybe 100 times less) to get the same effect as heroin. That is why drug cartels like it: they can make it cheap and don’t need to use as much of it= more profit for them. People aren’t that exact though – they are using more than they would need to get the ‘exact same effect’ as heroin. It’s why overdoses are so much more common when fentanyl is present. So in our thought experiment it is almost like we have 2 fentanyls sitting in each chair where we would have had only 1 heroin. Our theater now looks like this:
You can see the problem. Even in severe withdrawal there are not a lot of open seats for buprenorphine to sit in! It is going to have to push some fentanyl out of the way even though the person ALREADY feels AWFUL. Also remember that in heavy users some fentanyl will be slowly leaking back in from the fat stores. So some fentanyl people just keep wandering back in and sitting in the chairs you are trying to empty out. CURSES!
Stimulants and Xylazine
The use of stimulants and xylazine with a lot of fentanyl products further complicates the picture. Stimulant withdrawal can be kind of sneaky. Withdrawal in severe opioid addiction has a lot of symptoms: restlessness, anxiety, yawning, cramping, goosebumps, vomiting, diarrhea.
But stimulant withdrawal may not have as many physical symptoms. What it DOES do is mess with your mood and mind. A lot. I like to imagine that your brain is a tube of toothpaste where the toothpaste is made of the chemicals that help you feel ok/good. Methamphetamine forces your brain to release a lot more of those chemicals at once- it squeezes all the toothpaste out in one go. So, the next day you drop into depression/ irritability/anxiety and have no ‘toothpaste’ to help- you have to make more feel good chemicals and this takes some time (the worst withdrawal is the first 3-14 days). What this means is that if someone is withdrawing from fentanyl AND stimulants, their anxiety and irritability and feeling BAD is going to be EVEN WORSE. It was already hard enough to deal with ‘just’ bad opioid withdrawal and now we add on this extra weight?!
Xylazine has a similar problem. Xylazine is something mixed into opioids that many persons may not even know they are getting, much less how much they are getting. Withdrawal from xylazine results in high levels of agitation, anxiety, and possibly blood pressure changes. Furthermore, the buprenorphine is not going to help this part- buprenorphine doesn’t affect the same receptors that xylazine does. People withdrawing from these additional substances are going to have an even more difficult time waiting out the time between last use of the full opioid and beginning buprenorphine. They are more likely to jump the gun or to start taking other stuff (meth, coke, benzos) in addition to the buprenorphine that can affect the induction.
So, What Do We Do? See Part 2.
Footnotes
Note: Pharmacokinetics and pharmacodynamics which describe how drugs interact with receptors and the body processes is cool but complicated stuff. It is a lot more complicated and weird than I have described it here.↩︎
Reuse
Citation
@online{barnes2025,
author = {Barnes, Erin},
title = {Why {Is} {Getting} on {Buprenorphine} {So} {HARD} {These}
{Days?!} : {Part} 1},
date = {2025-11-13},
url = {https://wakeforestid.com/posts/2025-11-13-why-is-getting-bup-so-hard-1/},
doi = {10.59350/b7psw-sn910},
langid = {en}
}